Diverticulitis Treatment
 Our Diverticulitis treatment addresses the underlying issues, not just the symptoms. Treatment is carefully tailored to meet each patient’s unique needs.
Our Diverticulitis treatment addresses the underlying issues, not just the symptoms. Treatment is carefully tailored to meet each patient’s unique needs.
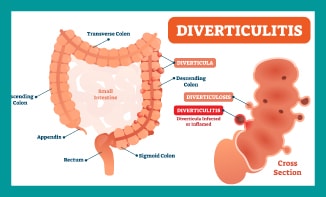
It is a condition where small, bulging pouches of the inner lining of the colon or large intestine (Diverticulosis) become inflamed or infected. According to orthodox medicine, no one knows exactly what causes the pouches to form in the first place. Eating a low-fibre diet is thought to be one of the most likely causes. In our approach to Diverticulitis treatment we aim to diagnose the underlying issues.
People who eat mostly processed food do not get enough fibre in their diet. Processed foods include white rice, white bread, most breakfast cereals, crackers, and pretzels. As a result, constipation and hard stools are more likely to occur – causing people to strain when passing stools. This increases the pressure in the colon or intestines and may cause these pouches to form.
Diverticulosis is very common. It is found in more than half of Americans over age 60. Diverticulitis is caused by small pieces of stool (faeces) that become trapped in these pouches, causing infection or inflammation.
People with diverticulosis are often without symptoms, but they may have bloating and cramping in the lower part of the abdomen. Rarely, they may notice blood in their stool or on toilet paper. Symptoms of diverticulitis are more severe and often start suddenly. Sometimes they may become worse over a few days.
They include:
- Tenderness, usually in the lower left side of the abdomen
- Bloating or excess gas
- Fever and chills
- Nausea
- Vomiting
- Loss of appetite
Patients are expected to have had a colonoscopy to rule out any serious disease. The underlying issues, which may have contributed to this condition, are diagnosed through medical tests and through taking an extensive case history. A Diverticulitis treatment plan is formulated based upon the patient’s test results. This personalised Functional Medicine approach usually works well and far better than a one-size-fits-all approach.
We also address any allergies that may be associated with this condition.
References
Diagnosis of symptomatic uncomplicated diverticular disease and the role of Rifaximin in management. Acta Biomed. 2017 Apr 28;88(1):25-32. doi: 10.23750/abm.v88i1.6360.PMID: 28467330 Free PMC article. Review.
If you would like an appointment
Contact Deborah’s Medical Secretary for an appointment